Housecall with Dr. David Doman has guest Dr. Mark Goldstein, Cancer Specialist on this episode discussing everything vital to Colon and Rectal Cancer management. The warning signs and symptoms, different screenings, varied scans, and clinical trials.
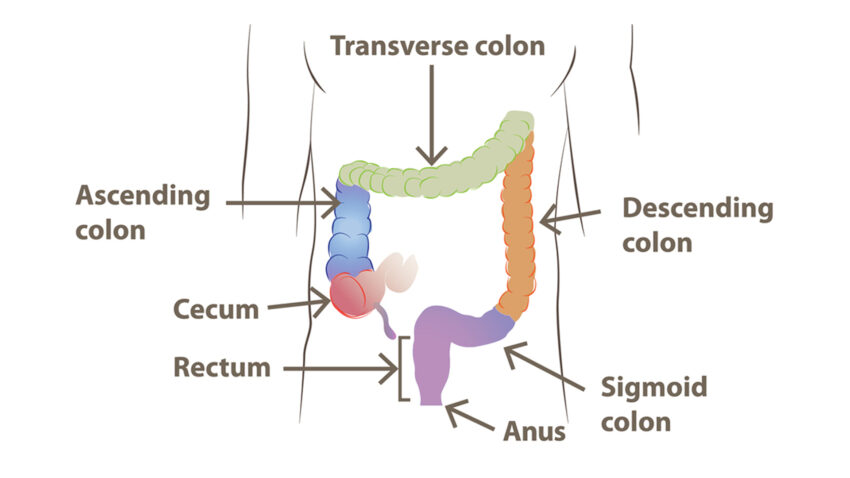
Symptoms depend on location of the cancer. If a patient has cancer in the first part of the colon in a liquid area, it may take some time to get symptoms, put they could include weight loss, sometimes pain. That’s why Colonoscopy are encouraged for screening. On the left side of the colon, further down by the rectum in a narrow area for stool to pass sometimes patient do have pain or pressure whether or not you’re moving your bowels.
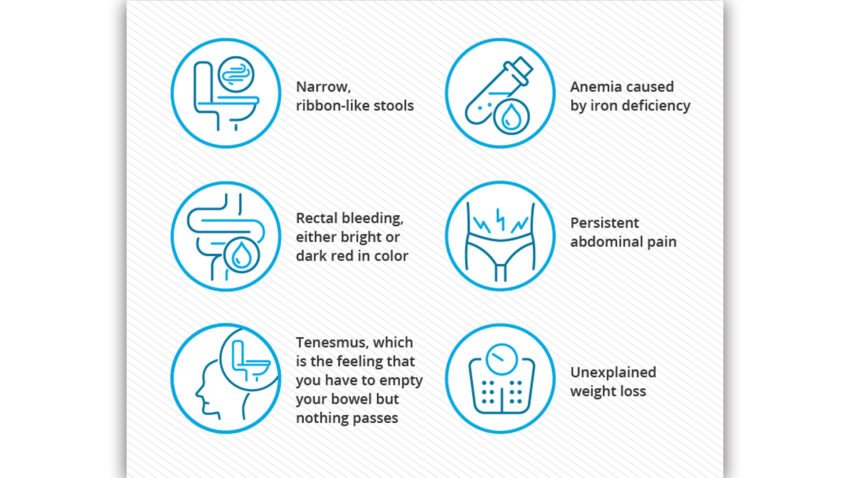
Warning Signs & Symptoms
Screenings available for Colorectal Cancer is Colonoscopy starting at age 45, most still think it is 50. Cologuard for average-risk patients. However, if there is significant family history of colon or rectal cancer, you can start at an earlier age. Galleri, a first of its kind which is a multi-cancer early detection test that looks for many (50+) cancers including many which are not commonly screened for today. Like 76.3% sensitivity in cancers that cause two-thirds of cancer deaths in the US. Plus, there is 99.5% specificity (very accurate for determining when a person did not have a cancer-related signal making False Positive results very unlikely.) In colon cancer + 11 other cancers combined,
Galleri finds about:
40% of stage I cancers,
67% of stage II cancers,
80% of stage III cancers and
95% of stage IV cancers.”
Average detection is about 67%
89% effective in predicting where the cancer started.
Most colon cancers and rectal cancers are adenocarcinoma. Adenocarcinoma is a type of cancer that starts in glands that line the insides of the organs, which is why it can affect different body areas. Adenocarcinoma forms in glandular epithelial cells, which secrete mucus, digestive juices or other fluids.

CT Scan
Colon cancer, CT scans are done to rule out metastatic disease. Then patients go for surgical resection. Some of those patients will require chemotherapy. However, specialized DNA testing performed a few weeks after resection may be able to determine who does not require chemotherapy. For example, 97% of patients who are ctDNA (+) at 4 weeks post-op will relapse without further treatment. These patients should receive chemotherapy. For rectal cancer, in addition to the CT scans, MRI of the pelvis is done to better characterize
the extent of disease to better stage the cancer. In the past, many patients underwent chemoradiation then surgery then chemo. What’s new is that we often utilize the TNT approach (Total Neoadjuvant Therapy) in which patients get chemotherapy then chemoradiation (or vice versa), then go to surgery. It is unclear whether or not some of those patients can avoid surgery if the restaging scans show no
CT vs MRI vs PET
CT scan of the chest/abd/pelvis are routine for staging of newly diagnosed patients with CRC.
-ideally, this requires iv and oral contrast; radiation exposure
-MRI pelvis is used for rectal cancer staging. Sometimes MRI is used to take a better look at the liver if CT is unrevealing but metastatic disease is still suspected. An alternative could be triple-phase CT of the liver.
The chemotherapy regimen we use today for colorectal cancers is similar to what we used 10 or more years ago, especially for patients who do not have metastatic (aka stage 4). However, some patients receive oral chemo only, or a combination of oral and iv chemo. Also, instead of 6 months of chemotherapy after surgery, many patients are now receiving only 3 months.
-for patients with advanced / metastatic / stage 4 colorectal cancer, we’ve been adding to standard chemo a variety of different antibodies, none of which are particularly new however
-in special circumstances we can use oral targeted medications rather than chemotherapy
Clinical Trials
Clinical trials are a very important part of the future of oncology. Some clinical trial are considered “first-in-human” but most are not. Most involve the study of new medications in combination with standard medications or in comparison with standard medications.
-for example in our office we have clinical trials for both metastatic rectal cancer and colon cancer patients; but we also have trials with simple blood work to monitor for recurrence of cancer.
-recurrences after initial treatment do happen. First we arrange for restaging scans to see all of the affected areas
-if there is a localized area, such as in the liver, we might decide to remove it with surgery or treat it directly; if the cancer is spread to multiple areas, then we must use chemotherapy + monoclonal antibodies, or targeted drugs.
To learn more visit aoncology.com and watch this episode of Housecall below and subscribe!
Comments are closed.